
Dr. James Manos (MD)
January 5, 2016
Review: Tips in Medical Biochemistry
Volume (10)
CONTENTS
SERUM PROTEIN ELECTROPHORESIS
Serum protein electrophoresis (SPEP or SPE)
Serum protein electrophoresis (SPEP) – causes of increased or decreased levels of serum protein fractions
Characteristic Features of Monoclonal Gammopathies
Urine Protein Electrophoresis
Bence Jones protein (urine)
Serum and Urine Immunofixation Electrophoresis (IFE)
Images for serum protein electrophoresis (SPEP)
Diagnostic algorithm for evaluation of an abnormal serum protein electrophoresis (SPEP)
SERUM PROTEIN ELECTROPHORESIS (SPEP or SPE)
· Serum protein electrophoresis (SPEP or SPE) is a laboratory test that examines the globulins (proteins in the blood).
· Electrophoresis is a laboratory technique in which the blood serum (the fluid portion of the blood after the blood has clotted) is placed into a gel, or into liquid in a capillary tube, and exposed to an electric current to separate the serum protein components into five major fractions by size and electrical charge: serum albumin, alpha – 1 globulins, alpha – 2 globulins, beta globulins, and gamma globulins.
{kind=link}
{kind=link}
· Images of normal serum protein electrophoresis (SPEP):
{kind=link}
{kind=link}
· Serum protein electrophoresis (SPEP) – causes of increased or decreased levels of a serum protein fractions:
· a) Albumin:
· Albumin is the major fraction in a normal SPEP. A fall of 30% is necessary before the decrease shows on electrophoresis. Usually, a single band is seen.
· Heterozygous individuals may produce bisalbuminemia – two equally staining bands, the product of two genes.
· Absence of albumin, known as analbuminaemia, is rare.
· i) Increased albumin: severe dehydration.
· ii) Decreased albumin: malnutrition, malabsorption, cachexia, liver disease (decreased albumin synthesis), renal disease (especially nephrotic syndrome), protein-losing enteropathies, severe burns, chronic infections, inflammatory conditions, hemorrhage, pregnancy.
{kind=link}
· b) Albumin – alpha 1 Interzone: even staining in this zone is due to alpha-1 lipoprotein (HDL; high-density lipoprotein).
· i) Decrease occurs in severe inflammation, acute hepatitis, cirrhosis, and nephrotic syndrome (loss of albumin through a damaged, leaky glomerulus).
· ii) An increase appears in severe alcoholics and women during pregnancy and in puberty.
· Note: The high levels of AFP (alpha-fetoprotein) that may occur in hepatocellular carcinoma may result in a sharp band between the albumin and the alpha-1 zone.
· c) Alpha – 1 fraction [alpha – 1 anti-trypsin (AAT), thyroid-binding globulin (TBG), transcortin (also known as corticosteroid-binding globulin (CBG) or serpin A6), alpha – 1 lipoprotein/ HDL (high-density lipoprotein), and alpha – 1 – acid glycoprotein (orosomucoid)]:
· alpha 1 – zone comprises alpha – 1 anti-trypsin (AAT), thyroid-binding globulin (TBG), transcortin [also known as corticosteroid-binding globulin (CBG) or serpin A6], alpha – 1 lipoprotein/ HDL (high-density lipoprotein), and alpha – 1 – acid glycoprotein (orosomucoid). Orosomucoid & antitrypsin migrate together but orosomucoid stains poorly so alpha – 1 anti-trypsin (AAT) constitutes most of the alpha-1 band.
· i) Increased alpha – 1 fraction: acute & chronic inflammatory diseases, pregnancy. As a positive acute phase reactant, AAT is increased in acute inflammation.
· Moreover, Bence Jones protein may bind to and retard the alpha-1 band.
{kind=link}
{kind=link}
· A normal alpha-2 and an elevated alpha-1 zone is a typical pattern in hepatic (liver) metastasis & cirrhosis.
· ii) Decreased alpha – 1 fraction: alpha – 1 antitrypsin deficiency (causes congenital emphysema), severe liver disease. A decreased or absent band is seen in alpha 1-antitrypsin deficiency. This condition eventually leads to pulmonary emphysema from unregulated neutrophil elastase activity in the lung tissue.
{kind=link}
{kind=link}
· The alpha-1 fraction does not disappear in alpha 1-antitrypsin deficiency, however, because other proteins, including alpha – lipoprotein and orosomucoid, also migrate there.
d) alpha – 1 – alpha – 2 Interzone. Two faint bands may be seen representing alpha-1 antichymotrypsin and vitamin D binding protein.
· These bands fuse and intensify in early inflammation due to an increase in alpha-1 antichymotrypsin, an acute-phase protein.
· e) Alpha – 2 fraction [alpha – 2 macroglobulin (AMG or A2M), haptoglobin, alpha – 2 antiplasmin, fibronectin, and ceruloplasmin]:
· alpha 2 zone consists principally of alpha – 2 macroglobulin (AMG or A2M) and haptoglobin, alpha – 2 antiplasmins, fibronectin, and ceruloplasmin.
· Haptoglobin is raised as part of the acute phase response, resulting in a typical elevation in the alpha-2 zone during inflammation.
· A normal alpha-2 and an elevated alpha-1 zone is a typical pattern in hepatic (liver) metastasis & cirrhosis.
· i) Increased alpha – 2 fraction: acute & chronic inflammatory diseases, nephrotic syndrome, oral contraceptive use, steroid use, hyperthyroidism, adrenal insufficiency, corticosteroid therapy, advanced diabetes mellitus.
· Alpha-2 macroglobulin may be elevated in children and the elderly. This αlso has a sharp front to the alpha-2 band.
· AMG is markedly raised (10-fold increase or higher) in association with glomerular protein loss, as in nephrotic syndrome (due to its large size, AMG cannot pass through glomeruli, while other lower-molecular-weight proteins show; so enhanced synthesis of AMG accounts for its absolute increase in nephrotic syndrome).
· AMG is mildly elevated early in the course of diabetic nephropathy.
· ii) Decreased alpha – 2 fraction: hemolysis/ hemolytic anemia (haptoglobin binds with hemoglobin released by red blood cells, and the complexes are moved by phagocytes rapidly), severe liver disease, malnutrition.
· f) alpha 2 – beta - Interzone: Cold insoluble globulin forms a band here which is not seen in the plasma because it is precipitated by heparin.
· i) There are low levels in inflammation and high levels in pregnancy.
· Beta lipoprotein forms an irregular crenated band in this zone.
· ii)High levels are seen in type II hypercholesterolemia, hypertriglyceridemia, and nephrotic syndrome.
· g) Beta fraction [beta – 1: transferrin; beta – 2: beta-lipoprotein (LDL; low-density lipoprotein) and fibrinogen; IgA, IgM, and sometimes IgG, along with complement proteins such as c3 & c4, also can be identified in the beta fraction]:
· Βeta – 1 zone comprises transferrin. Beta – 2 zone includes beta-lipoprotein (LDL; low-density lipoprotein) and fibrinogen.
· Beta-2 comprises C3 (complement protein 3)
· IgA, IgM, and sometimes IgG, along with complement proteins, also can be identified in the beta fraction.
· i) Increased beta fraction (beta 1 or beta 2): hyperlipidemia, iron deficiency anemia, biliary cirrhosis, carcinoma (sometimes), Cushing’s disease, diabetes mellitus (some cases), hypothyroidism, nephrosis (nephrotic syndrome), malignant hypertension, polyarteritis nodosa, obstructive jaundice, pregnancy (3rd trimester). Note: beta fraction may also be increased in some cases of multiple myeloma or monoclonal gammopathy of unknown significance (MGUS).
· Increased beta-1 protein due to the increased level of free transferrin is typical of iron deficiency anemia, pregnancy, and estrogen therapy.
· Increased beta-1 protein due to LDL elevation occurs in hypercholesterolemia.
· Beta-2 comprises C3 (complement protein 3) that is raised in the acute phase response.
· Fibrinogen, a beta-2 protein, is found in normal plasma but is absent in normal serum. Occasionally, blood drawn from heparinized patients does not fully clot, resulting in a visible fibrinogen band between the beta and gamma globulins.
{kind=link}
· ii) Decreased beta fraction (beta 1 or beta 2): hypo – B – lipoproteinemia, liver cirrhosis, (protein) malnutrition.
· Decreased beta-1 protein occurs in acute or chronic inflammation.
· Beta-2 comprises C3 (complement protein 3). Depression of C3 occurs in autoimmune disorders as the complement system is activated and the C3 becomes bound to immune complexes and removed from the plasma.
· h) Beta – gamma Interzone: CRP (C – reactive protein) is found in between the beta and gamma zones producing beta/gamma fusion.
· IgA immunoglobulin has the most anodal mobility and migrates in the region between the beta and gamma zones also causing a beta/gamma fusion in patients with cirrhosis, respiratory infection, skin disease, or rheumatoid arthritis (increased IgA).
· CRP is an acute-phase protein produced by the liver the levels of which rise in response to inflammation.
· i) Gamma fraction [immunoglobulins (IgA, IgM, IgG, IgE, and IgD).
· Note: It should be noted that immunoglobulins often can be found throughout the electrophoretic spectrum].
· The immunoglobulins (IgA, IgM, IgG, IgE, and IgD) are the only proteins present in the normal gamma region. However, they may be found in the alpha and beta zones.
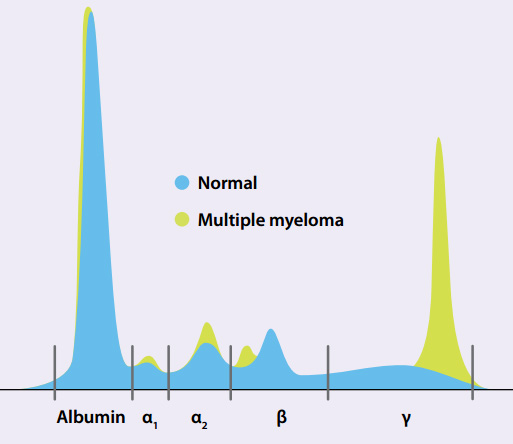
· If the gamma zone shows an increase (or spike), the first step in interpretation is to establish if the region is narrow or wide. If it is elevated in a single narrow “spike-like” manner, it could indicate monoclonal production of a single immunoglobulin (monoclonal gammopathy), while a broad “swell-like” manner (wide) indicates polyclonal immunoglobulin production.
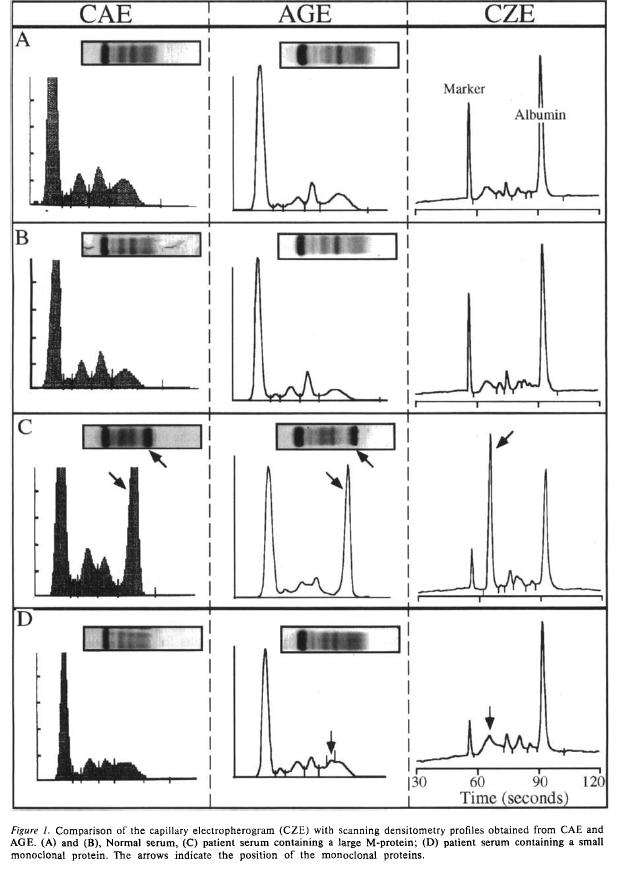
· Immunofixation (gel electrophoresis) or immunosubtraction (capillary electrophoresis) are performed to detect and confirm monoclonal immunoglobulins.
· a) Increased gamma fraction:
· A) Polyclonal gammopathies.
· A “swell-like” elevation in the gamma zone indicates a polyclonal gammopathy, which typically indicates a non-neoplastic condition (although is not exclusive to non-neoplastic conditions).
· A broad – higher increase of gamma zone indicates polyclonal immunoglobulin production. Causes: severe infection, chronic infections – granulomatous diseases, chronic liver disease (e.g. cirrhosis, ethanol abuse, autoimmune hepatitis, viral-induced hepatitis, primary biliary cirrhosis, primary sclerosing cholangitis), autoimmune diseases & connective tissue diseases (e.g. rheumatoid arthritis, mixed connective tissue, temporal arteritis, systemic lupus erythematosus (SLE), sarcoid and other) and recent immunization. Also, other medical conditions that may cause a polyclonal rise in the gamma fraction include chronic viral infections (especially hepatitis, HIV, infectious mononucleosis, varicella) or bacterial infections (including endocarditis, osteomyelitis, and bacteremia), tuberculosis, various malignancies (e.g. solid tumors, ovarian tumors, lung cancer, hepatocellular cancer, renal tumors, gastric tumors, hematologic cancers), hematologic (e.g. thalassemia, sickle cell anemia) and lymphoproliferative disorders (e.g. lymphoma, leukemia), and other inflammatory conditions (e.g. gastrointestinal conditions, including ulcerative colitis and Crohn’s disease; pulmonary disorders, including bronchiectasis, cystic fibrosis, chronic bronchitis, and pneumonitis; endocrine diseases, including Graves’ disease and Hashimoto's thyroiditis).
{kind=link}
· http://synapse.koreamed.org/ArticleImage/0052KJP/kjped-56-304-g002-l.jpg (full article: http://synapse.koreamed.org/DOIx.php?id=10.3345/kjp.2013.56.7.304&vmode=PUBREADER )
{kind=link}
· B) Monoclonal gammopathies (also called paraproteinemias). A narrow spike indicates a monoclonal gammopathy, also known as an “M-spike”.
· Typically, a monoclonal gammopathy is malignant or clonal in origin. Multiple myeloma is the most common cause of IgA and IgG spikes.
· Chronic lymphatic leukemia and lymphosarcoma are not uncommon and usually give rise to IgM paraproteins.
· Note: up to 8% of healthy geriatric patients may have a monoclonal spike.
· Μ – spike is also seen in Waldenstrom’s macroglobulinemia (IgM spike), monoclonal gammopathy of undetermined significance (MGUS), amyloidosis, plasma cell leukemia, and solitary plasmacytomas.
{kind=link}
{kind=link}
· Causes of monoclonal gammopathy: usually caused by an underlying immunoproliferative disorder; causes: e.g. multiple myeloma, smoldering myeloma, Castleman disease, heavy-chain deposition disease, light chain deposition disease, plasmacytoma, lymphoplasmacytic lymphoma, leukemias & lymphomas (usually B – cell Non – Hodgkin’s lymphomas with a plasma cell component), Waldenstrom’s macroglobulinemia (IgM spike), monoclonal gammopathy of undetermined significance (MGUS), and primary systemic (AL) amyloidosis (only light chains).
· Note: Castleman disease (also known as giant or angiofollicular lymph node hyperplasia, lymphoid hamartoma, angiofollicular lymph node hyperplasia) is a group of uncommon lymphoproliferative disorders that share common lymph node histological features that may be localized to a single lymph node (unicentric) or occur systemically (multicentric). Hypersecretion of cytokines causes lymph node abnormalities and organ dysfunction in Castleman disease, commonly IL – 6. The release of these cytokines is caused by HHV-8 (human herpesvirus; also known as Kaposi's sarcoma-associated herpesvirus (KSHV) that causes sarcoma Kaposi, commonly in AIDS patients, and primary effusion lymphoma) in HHV-8-associated MCD. It MCD clinical features range from waxing and waning mild lymphadenopathy with B-symptoms to more severe cases involving intense inflammation, generalized lymphadenopathy, hepatosplenomegaly, vascular leak syndrome with anasarca, pleural effusions, and ascites, organ failure, and even death. The most common ‘B Symptoms’ of MCD are high fevers, night sweats, weight loss, and loss of appetite. Laboratory findings commonly include low red cell count, low or high platelet counts, low albumin, high gamma globulin levels, elevated CRP levels, elevated ESR, IL-6, vascular endothelial growth factor (VEGF), and fibrinogen; positive ANA (anti-nuclear antibody), anti-erythrocyte autoantibodies, and antiplatelet antibodies; and proteinuria and polyclonal marrow plasmacytosis. Castleman disease is seen in POEMS syndrome (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes) and is implicated in 10% of cases of paraneoplastic pemphigus (a skin disease, usually blisters, related to cancer that triggers it as an autoimmune response).
· Monoclonal increase in gamma region may also occur on POEMS syndrome (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes).
· Also, an M component may be detected in other lymphoid malignancies like chronic lymphocytic leukemia, any B- or T- cell lymphomas, breast cancer, colon cancer, cirrhosis, sarcoidosis, and other autoimmune disorders.
· Increased gamma globulins may also occur in Hodgkin’s disease and CLL (chronic lymphocytic leukemia).
· Paraproteinemias may be categorized according to the type of monoclonal protein found in the blood:
· a) Light chains only (or Bence Jones protein): may be associated with multiple myeloma or AL amyloidosis (primary systemic amyloidosis).
· b) Heavy chains: heavy chain disease.
· c) Whole immunoglobulins: the paraprotein goes under the name of “M-protein” (“M” for monoclonal). If immunoglobulins tend to precipitate within blood vessels with cold, that phenomenon takes the name of cryoglobulinemia.
· Other paraproteins may increase blood viscosity (usually with IgM macroglobulins) such as Waldenstrom macroglobulinemia.
· Note: Monoclonal proteins are produced by one clone of plasma cells, and thus all the molecules are identical and have the same electrical charge. That is why on electrophoresis a monoclonal protein will migrate as a narrow spike called M spike. This spike appears most often in the gamma zone, but sometimes can be present in Beta 2 or Beta 1, or even the Alpha 2 zone, although the latter is scarce.
{kind=link}
{kind=link}
· b) Decreased gamma fraction: agammaglobulinemia, hypogammaglobulinemia.
· Hypogammaglobulinaemia is easily identifiable as a “slump” or decrease in the gamma zone. It is normal in infants. It is found in patients with X – linked agammaglobulinemia. IgA deficiency occurs in 1:500 of the population, as is suggested by a pallor in the gamma zone. Lysozyme may be seen as a band cathodal to the slowest gamma in myelomonocytic leukemia in which it is released from tumor cells. Fibrinogen from plasma samples will be seen in the fast gamma region.
{kind=link}
· For serum protein electrophoresis see also:
· Characteristic Features of Monoclonal Gammopathies:
· a) Multiple myeloma: M protein appears as a narrow spike in the gamma, beta, or alpha 2 regions; M-protein level is usually greater than 3 g/dL; skeletal lesions (e.g., lytic lesions, diffuse osteopenia, vertebral compression fractures) are present in 80%; diagnosis requires 10 – 15% plasma cell involvement on bone marrow biopsy; anemia, pancytopenia, hypercalcemia, and renal disease may be present.
· b) Monoclonal gammopathy of undetermined significance (MGUS): M-protein level is less than 3 g/dL; there is less than 10% plasma cell involvement on bone marrow biopsy; affected patients have no M protein in their urine, no lytic bone lesions, no anemia, no hypercalcemia, and no renal disease.
· c) Smoldering multiple myeloma: M-protein level is greater than 3 g/dL; there is greater than 10% plasma cell involvement on bone marrow biopsy; affected patients have no lytic bone lesions, no anemia, no hypercalcemia, and no renal disease.
· d) Plasma cell leukemia: peripheral blood contains more than 20% plasma cells; M-protein levels are low; affected patients have few bone lesions and few hematologic disturbances; this monoclonal gammopathy occurs in younger patients.
· e) Solitary plasmacytoma: affected patients have only one tumor, with no other bone lesions and no urine or serum abnormalities.
· f) Waldenstrom’s macroglobulinemia: IgM M protein is present; Affected patients have hyperviscosity and hypercellular bone marrow with extensive infiltration by lymphoplasma cells.
· g) Heavy chain disease: the M protein has an incomplete heavy chain and no light chain.
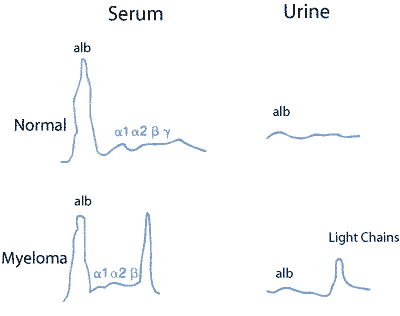
· Urine Protein Electrophoresis: the kidney acts as a filter, eliminating only a few molecules and leaving most of the proteins in the bloodstream. Although some small proteins do pass through the kidney filter, they are later resorbed and recycled into amino acids. Thus, normal urine contains only traces of proteins. When monoclonal protein is present in serum, often the excess of free light chains will be found in the urine as Bence Jones protein (it will look like a narrow spike, usually in the gamma or beta zone). Urine protein electrophoresis is used to search for Bence Jones protein and to monitor its concentration. It can also help to assess kidney damage (which is a common complication of multiple myeloma)
{kind=link}
{kind=link}
· Bence Jones protein (urine): a monoclonal globulin protein or immunoglobulin light chain found in urine, with a molecular weight of 22-24 kDa. The Bence – Jones protein refers to an immunoglobulin light chain. The Bence – Jones protein is secreted into the urine where it can be measured.
· Detection of Bence Jones protein may be suggestive of multiple myeloma or Waldenstrom's macroglobulinemia. Bence Jones proteins are particularly diagnostic of multiple myeloma in the context of end-organ manifestations such as renal failure, lytic (or "punched out") bone lesions, anemia, or large numbers of plasma cells in the bone marrow of the patients. Bence Jones proteins are present in 2/3 of multiple myeloma cases. Patients with plasmacytomas, such as patients with multiple myeloma, overproduce monoclonal immunoglobulins, called M proteins.
· Sometimes (on a pure light chain myeloma) the only M spike is on the urine:
· Serum and Urine Immunofixation Electrophoresis (IFE): Once a narrow spike of protein is detected by protein electrophoresis, the presence of monoclonal protein may be suspected. It is necessary then to confirm its presence and to determine its type by identifying which types of heavy chains and light chains are involved in its structure. Knowing the type of M-protein is important in establishing a diagnosis and in monitoring the patient. To do this, another method of electrophoresis, called immunofixation (or IFE, for Immunofixation Electrophoresis), will be used.
· Immunofixation identifies the type of immunoglobulin protein(s) present in monoclonal bands on a protein electrophoresis pattern; typically immunofixation determines the presence of a heavy chain (IgG, IgM or IgA) and a light chain (kappa or lambda). Immunofixation methods are more sensitive to the presence of faint monoclonal proteins and may detect them even if electrophoresis does not show any visible abnormality. But immunofixation does not determine how much M-protein is present. Therefore, both methods are used together: electrophoresis to detect the monoclonal protein and to quantify it, and immunofixation to identify its type.
· Images for serum protein electrophoresis (SPEP):
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
· Diagnostic algorithm for evaluation of an abnormal serum protein electrophoresis (SPEP):
{kind=link}
No comments:
Post a Comment